“The services provided by Pet Dental Services have proven to be invaluable to our practice. Our clients appreciate the safety and convenience that non-anesthetic dentistry provides to their pets. Pet Dental Service’s staff is incredibly kind and patient with the pets in their care. Even some of our fearful patients are able to benefit from a full dental cleaning due to the gentle care provided by the PDS staff.”
-
 Dr. Melissa Byers
Lake Forest Animal Clinic
Lake Forest, CA
Dr. Melissa Byers
Lake Forest Animal Clinic
Lake Forest, CA
-
“Their technique is gentle yet so very effective in the patients that qualify for this procedure. I have not encountered a case yet that I am not totally satisfied with the outcome. Having Pet Dental Services as part of your healthcare team is a win, win, win situation.”
Dr. Laurie Koorhan
Doctors Pet Clinic
Murrieta, CA
-
We have been very happy with the level of service we receive from Pet Dental Services, a teeth cleaning service without anesthesia for cats and dogs. They are very professional and relaiable. They are friendly and knowledgeable regarding dental cleaning, and are very good with our clients. They take the time to explain the procedure and are always willing to over the dental report with the client.
Their technicians arrive once per week (4 times per month) to our clinic, bringing with them all their own equipment. they perform a full teeth cleaning with manual polishing and complete charting, which the client gets a copy of. They typically service between 80 and 100 patients per month at our facility.
The level of professional care can be seen by us as well as the clients, which keeps most of them booking repeat cleanings for their pets on a regular basis.
We would be more than happy to recommend Pet Dental Services to any veterinary clinic or animal care facility.
Eric Christensen
Hospital Administrator
Founders Veterinary Clinic
-
“Since day one working with the Pet Dental Services crew, we have been impressed with their ease handling our numerous film animals, and the undeniable fact that our dental costs have reduced significantly.”
Birds & Animals Unlimited are the owners and trainers of numerous film animals including Moose from “Frasier”, Laiko from “Because of Winn Dixie”, Pongo & Perdy from “101 & 102 Dalmatians”, Coal from “The Shaggy Dog”, just to name a few.
Lorraine Putnam
Operations Manager
Birds & Animals Unlimited
-
I have been using the non anesthetic dental cleaning treatments for approximately seven years now and they work great. They are in no way intended to take the place of deep cleaning, extractions and radiographs that are all done during anesthetic dentals. They are an excellent complement to thorough dental care. Once a deep cleaning is done with anesthesia, a follow up preventative cleaning is scheduled in 4 to 6 months to maintain the teeth in great health. Younger dogs with no major dental disease can be scheduled for non anesthetic dentals to prevent the tartar buildup and gingivitis. They are to be used as we do with people, routine dental cleanings to prevent severe dental disease. The non anesthetic dentals if started early in the life of our pets, followed up with good home care can prevent a lot of problems in the future. They are also a great alternative for the geriatric pet that has a greater risk with anesthesia. The advantage with the geriatric pet is greater if dental cleaning has already been instituted in the past when the pet was in good health.
Dr. Cristina Comartin
-
“I was very happy with the cleaning that the technician did.”
Ethel Levine
-
“The technician was absolutely fantastic at educating me on my pet’s dental health.”
C.L.
-
“I would definitely recommend Pet Dental Service to my family and friends.”
Michelle O’Keefe
-
“The PDS technician thoroughly explained my pet’s dental health needs.”
S.J.
-
“The technician was thorough, kind and clearly she loves the animals with whom she works.”
Erica Simba
-
“If Pet Dental Services was a hotel, I would give you 5 stars.”
Erica Melville
-
“I would absolutely recommend Pet Dental Services to my friends and family.”
S.J.
-
“The technician was fantastic, very educated and all around it was a great experience.”
Jenny McKell
-
“The technician had great communication over the phone.”
Jeanette Orlen
-
“I was educated on my pet’s dental health needs by the technician, and I would recommend Pet Dental Services to my friends and family.”
P.P.
-
“I feel this service really keeps my pet’s breath fresh”
Cheryl Rice
-
“The technician was excellent! She explained everything and kept me updated.”
Ann Marie Gamble
-
“The technician gave very helpful tips on the techniques for brushing our dog’s teeth. I was amazed that he wagged his tail through the whole cleaning!”
Shirley McCray
-
“The technician was very thorough in her communication.”
Barbara Elliot
-
“The technician was very educational and I am very happy.”
H.Z.
-
“I have seen what dental neglect can do, and this procedure is very beneficial.”
B.F.
-
“Better health and a happy babygirl make this service so beneficial.”
J.S.
-
“I love the result of the cleaning, the friendly technicians and that my dog is not frightened.”
Colleen Dickson
-
“Without this service, my dog would be in serious trouble with bacterial infections.”
Sylvia Crockett
-
“The technician was very gentle with my Dachshund and explained the at home cleaning process thoroughly.”
John James
-
“I love that I don’t have to sedate my dog! Her appointment was right on time and the technician was very kind and honest.”
Jessica Lawson
-
“I have a fussy dog who doesn’t like her mouth touched and the PDS technician was able to successfully and thoroughly clean her teeth.”
Christie Lesinski
-
“The researchers were able to identify all areas of pathology, and confirmed their findings with radiography. Therefore, their research supports the conclusion that a probing and cleaning can be done without general anesthesia.”
Patrick Hardigan Ph. D.
-
“I have been using Pet Dental Services for the past 3 years. Not only is the staff courteous and professional, but the extent of the work being done is superlative. Since we have started offering this lower cost non-anesthetic option, client compliance has begun to improve. It is a win/win situation, pets that are eligible for this non-anesthetic procedure are getting the dental care that is essential for their overall health and clients are benefiting from getting affordable preventative care. Also, some clients are extremely sensitive to placing their pet under anesthesia. It is a pleasure being able to satisfy the clients, but also give the pet the care they deserve.”
Brian Gerard, D.V.M.
-
“The technician is always helpful, professional and on time.”
Terry Archer
-
“If I hadn’t had the dental scheduled with Pet Dental Services, I don’t think the nasal growth would have been found.”
F.L.

News & Updates
All News & Updates


News & Updates
Enter your email below to receive coupons, the latest PDS news, and tips and tricks for caring for your pet's teeth.
Download Brochure (PDF)
Show this brochure
to your vet and
request our service
in your hospital.
Study on Professional Outpatient Preventative Dentistry (POPD)
September 24, 2013
Can it be done safely and effectively without the use of general anesthesia?
By Mayra Urbieta, DMD, Stephanie Sur, DVM, Patrick Hardigan, PhD, Darren Pike, DMD, MS and Chad Orlich, DMD
A double-blind study of 12 dogs and 12 cats, randomly selected and divided by age group and history of anesthetic dental treatment, were used in the study. Subjects were treated with an experimental intervention (POPD) by a trained Pet Dental Services (PDS) technician and subsequently examined under general anesthesia by a board-certifi ed veterinary dentist (control). The examination consisted of inspection for any remaining subgingival calculus using compressed air, exposed full mouth radiographs and a complete oral exam. Parameters examined by both groups included recession, furcation, hyperplasia, resorption, missing teeth, fractures/attrition/ abrasion, supernumerary teeth, and probing depths.
 Results showed that the trained technicians and the veterinary dentist were both able to identify the seven dental conditions, although the technician appeared to report more pathology. After the POPD was successfully completed, no residual plaque or calculus was detected on any of the dogs or cats and there were no post-treatment complications. Although a POPD is not intended to be a substitute for anesthetic dentistry, it may prove to be a valuable supplemental treatment. The methods for the study included fi rst grouping the 24 animals by age and prior dentistry within the preceding two years. All were examined by a board certifi ed veterinary dentist to determine the appropriateness of a POPD, and evaluated with lab work to determine eligibility for general anesthesia. All subjects were deemed to be healthy and capable of undergoing the procedures required for this trial. The experimental intervention (POPD) was performed on all patients by PDS technicians who are qualifi ed by examination from the American Society of Veterinary Dental Technicians (ASVDT), First Aid/CPR certifi ed by the American Red Cross, and with a minimum of three years of experience working in a veterinary hospital. They were instructed over a six-month period, with a training program developed in part by a boardcertifi ed periodontist and PDS, and overseen by multiple veterinarians.
Results showed that the trained technicians and the veterinary dentist were both able to identify the seven dental conditions, although the technician appeared to report more pathology. After the POPD was successfully completed, no residual plaque or calculus was detected on any of the dogs or cats and there were no post-treatment complications. Although a POPD is not intended to be a substitute for anesthetic dentistry, it may prove to be a valuable supplemental treatment. The methods for the study included fi rst grouping the 24 animals by age and prior dentistry within the preceding two years. All were examined by a board certifi ed veterinary dentist to determine the appropriateness of a POPD, and evaluated with lab work to determine eligibility for general anesthesia. All subjects were deemed to be healthy and capable of undergoing the procedures required for this trial. The experimental intervention (POPD) was performed on all patients by PDS technicians who are qualifi ed by examination from the American Society of Veterinary Dental Technicians (ASVDT), First Aid/CPR certifi ed by the American Red Cross, and with a minimum of three years of experience working in a veterinary hospital. They were instructed over a six-month period, with a training program developed in part by a boardcertifi ed periodontist and PDS, and overseen by multiple veterinarians.
The POPD 11-step protocol used by PDS technicians follows; however, steps 3, 10 and 11 were omitted in order to maintain the double-blind study design.
STEP 1: Medical and behavioral history check.
STEP 2: Pre-exam – physical and oral. A check of joint discomfort or pain is conducted to determine a pet’s candidacy for the procedure since restraint is necessary during a POPD. A complete extra-oral and intra-oral exam is completed, with a specific focus on tooth symmetry, swelling and pain. An evaluation is also performed on each tooth, and surrounding gingiva, for pathology including calculus levels, compromised teeth, gingival condition and periodontal pockets. At this point, in a clinic setting, for 62.5% of the subjects, the technician would have stopped the procedure after the exam and discussed the findings with the veterinarian because he/she would be recommending an anesthetic dental treatment.
STEP 3: Treatment plan – a treatment plan is then generated through a staff-doctor-client partnership. Treatment plans can range from simply completing the POPD procedure to recommending that the professional oral hygiene procedure be performed under general anesthesia. The treatment plans include home care instructions and a recall date for an anesthetic dental treatment or a maintenance POPD procedure, if necessary. This step is crucial in ensuring the patient receives the proper care for his/her periodontal and health condition.
STEP 4: Supra-gingival scaling – a POPD begins with the removal of supra-gingival deposits of plaque and calculus from the buccal, lingual and interproximal surfaces. A combination of forceps, hand instruments and ultrasonic piezo scaling are used for plaque and calculus removal.
STEP 5: Sub-gingival scaling and curettage – plaque and calculus deposits are thoroughly removed from the sub-gingival areas. This procedure is not performed on a patient with stage three or four periodontal disease. This reinforces the need for a pre-examination (Step 2) for patient candidacy.
STEP 6: Post dental probing – a six-point probing of each tooth is performed. A thorough probing is vital for recognizing and communicating areas of concern to the doctors and clients. All abnormal pocket depths are noted for the final chart.
STEP 7: Machine polish – hygienists then perform a machine polish using a pumice or polishing paste. Polishing will assist in smoothing out minor defects of the enamel which may have occurred during the procedure, thus aiding in the prevention of future plaque accumulation. It will also help with the removal of certain enamel stains.
STEP 8: Oral rinse – any diseased tissue, plaque or paste remnants are removed through an irrigation of the oral cavity. The oral cavity and gingival pockets or sulcus are flushed with a chlorhexidine-based solution. 36 IVC Fall 2013
STEP 9: Post-check and charting – a complete evaluation of each tooth is performed, checking for any retained calculus with a periodontal probe and/or explorer. The dental chart is completed.
STEP 10: Veterinarian and staff communication – a veterinarian examines the oral cavity with a corresponding evaluation of the dental chart to ensure complete pathological notation. A posttreatment oral health care plan is prepared for the patient.
STEP 11: Client education – fi nally, the hygienist educates clients about the importance of maintaining good oral health in their pets. They will also review the pet’s dental experience and chart, review the importance of continuous recalls and explain to them the many options regarding home care. They also provide brushing demonstrations with their pet, when necessary.
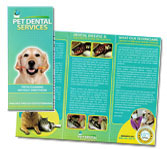
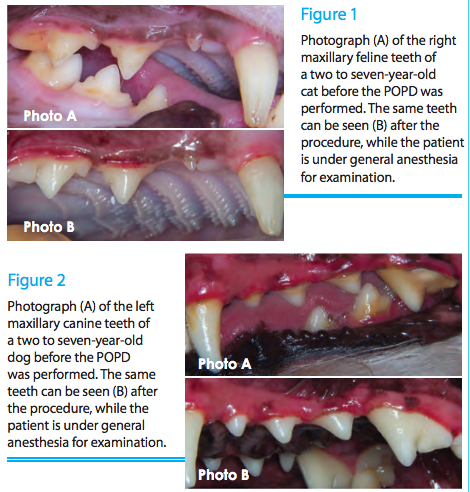 Following the completion of POPD treatment by the trained technician, all patients were immediately put under general anesthesia and examined thoroughly by a veterinarian. The veterinarian used compressed air to dry the gingival margins and properly inspect for any remaining subgingival calculus, exposed full mouth radiographs, and fi lled out a pre-designated chart. The same chart was used by the veterinarian for their pre-treatment examination. Also noted was gingival recession, furcation involvement, gingival hyperplasia, tooth resorption, missing teeth, supernumerary teeth, fractures/attrition/abrasion, and probing depths. The veterinary staff also took before and after pictures of each patient (See Figures 1 and 2 below for examples). All the patients for which the technician recommended anesthetic dental treatment were found to have radiographic fi ndings by the control group’s examination.
Following the completion of POPD treatment by the trained technician, all patients were immediately put under general anesthesia and examined thoroughly by a veterinarian. The veterinarian used compressed air to dry the gingival margins and properly inspect for any remaining subgingival calculus, exposed full mouth radiographs, and fi lled out a pre-designated chart. The same chart was used by the veterinarian for their pre-treatment examination. Also noted was gingival recession, furcation involvement, gingival hyperplasia, tooth resorption, missing teeth, supernumerary teeth, fractures/attrition/abrasion, and probing depths. The veterinary staff also took before and after pictures of each patient (See Figures 1 and 2 below for examples). All the patients for which the technician recommended anesthetic dental treatment were found to have radiographic fi ndings by the control group’s examination.
Discussion
Since plaque is the initiating cause of gingivitis and subsequent periodontitis, assessment of plaque reduction is a key step in determining the effi cacy of canine and feline dental health products and procedures. The present pilot study implies that performing a dental prophylaxis on a cat or dog without the use of general anesthesia can be done in a safe and effi cient manner by an appropriately trained technician. Not only were the dental prophylaxes completed on all 24 patients, but also there was no residual calculus remaining supra- or sub-gingivally upon thorough inspection by the veterinarian. In addition, there were no post-treatment complications, which again attest to the possibility of performing such a procedure in a safe manner. This procedure must be performed under the supervision of a licensed veterinarian. Therefore, it is crucial to keep in mind the scope of a procedure such as POPD. Like any other procedure performed by an auxiliary, POPD is to be used at the discretion of the veterinarian, for he or she is ultimately responsible for the overall health of each patient. It is not intended at any time to replace anesthetic dentistry, but to support it, meaning that it is up to the doctor to decide when and for what patients the service is appropriate. Also, it should be noted that if this were not a research setting, the technician would have stopped the POPD after the exam in 62.5% of the patients, all of which were also found to have radiographic fi ndings, and discussed the fi ndings with the veterinarian due to the nature of the present pathology.